Guidelines
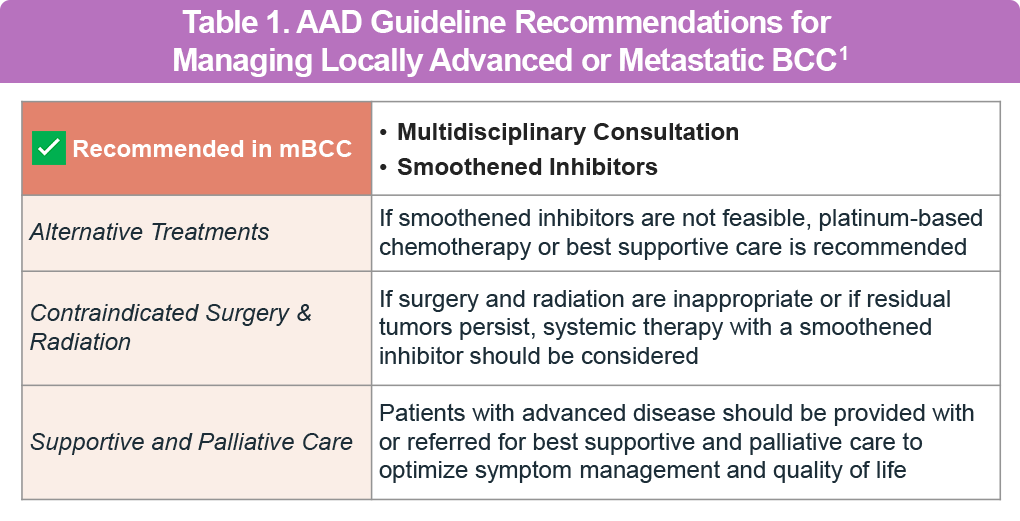
The evolving guidance from professional societies reflects the growing knowledge of the pathogenesis of non-melanoma skin cancers (NMSCs) and ongoing clinical research on systemic therapy for BCC. Several guidelines worldwide, including those from the National Comprehensive Cancer Network® (NCCN), American Academy of Dermatology (AAD), and European Association of Dermato-Oncology (EADO), recommend the use of Hedgehog inhibitors (HHIs) for “difficult-to-treat” BCC, such as locally advanced BCC (laBCC), metastatic BCC (mBCC), and Gorlin syndrome (Table 1). For patients with laBCC or mBCC that is relapsed or refractory to HHIs, or for those intolerant or unsuitable for HHIs, an approved anti-PD-1 therapy is recommended by the Society for Immunotherapy of Cancer (SITC) clinical practice guidelines.
Metastatic BCC is exceedingly rare, with an estimated incidence of 0.0028% to 0.55%, and has historically been associated with a very poor prognosis. The most common progression pathway involves lymphatic metastasis to regional lymph nodes, followed by hematogenous spread to the lungs and bones.1
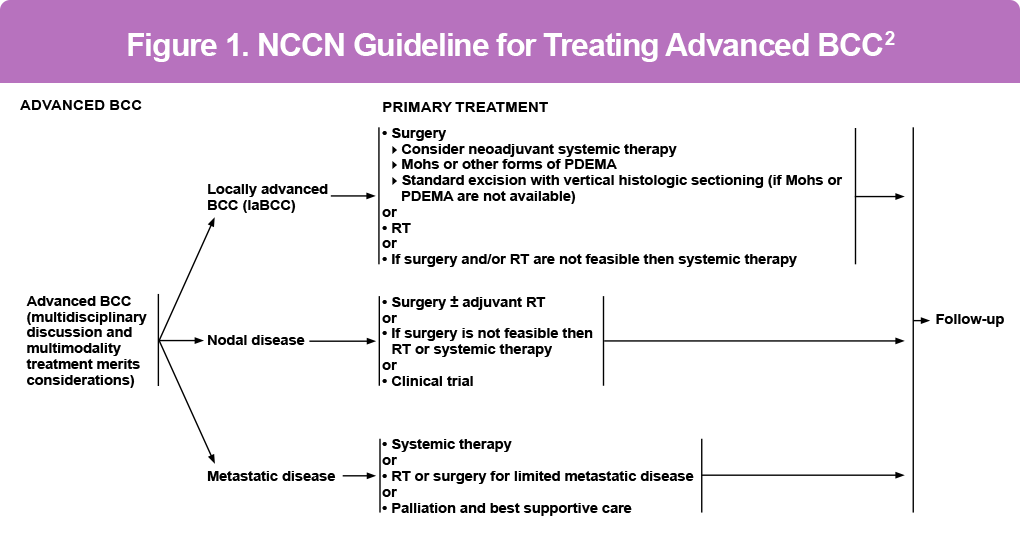
NCCN Guidelines for Treating Advanced BCC
The NCCN guidelines recommend a multidisciplinary approach to complicated cases of BCC (Figure 1). Treatment recommendations are based on the differentiation between localized tumors at low versus high risk for recurrence, considering both clinical and pathologic parameters.2
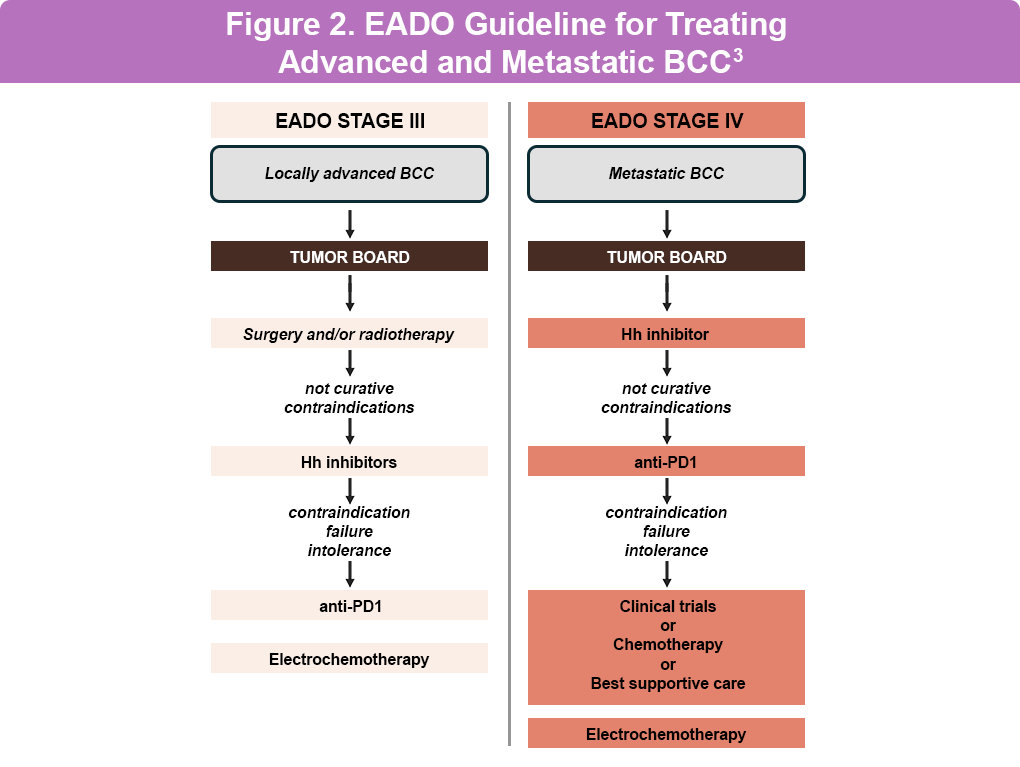
European Association of Dermato-Oncology (EADO) Guidelines for Treating Advanced and Metastatic BCC
The EADO guidelines align with other global recommendations, emphasizing the use of HHIs and systemic therapies for advanced BCC cases (Figure 2).3
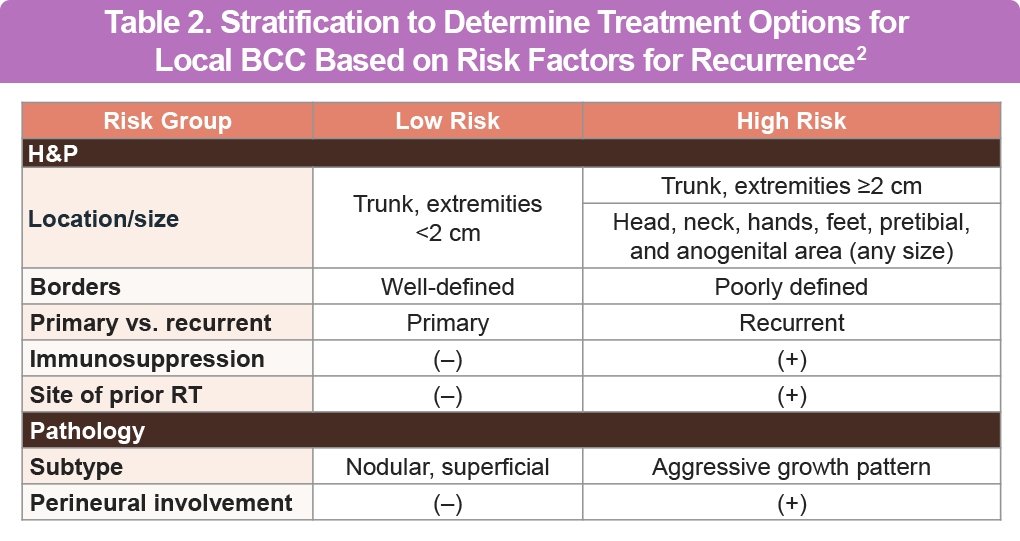
Risk Stratification for Local BCC
A formal staging system for BCC risk stratification is not available. The NCCN provides the most clinically relevant stratification, differentiating between low and high risk for recurrence. This stratification guides treatment recommendations based on available evidence and expert opinion from various medical specialties (Table 2).1
Research Gaps and Future Directions
Significant gaps in research remain regarding the optimal management of BCC, including the use of dermoscopy and imaging modalities for diagnosis, the clinical value of biomarkers, and the identification of noninvasive treatment modalities with recurrence rates comparable to surgery. Further research is needed to optimize systemic inhibitors of the Hedgehog pathway and develop novel therapies with high response rates and tolerable side effect profiles.1
The management of BCC should always be tailored to individual patient needs, the latest evidence, and expert consensus. Continuous research and updated guidelines are crucial to improving patient outcomes and advancing the understanding of BCC treatment.
References
- Work Group; Invited Reviewers, Kim JYS, et al. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78:540-559. doi:10.1016/j.jaad.2017.10.006
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology. Basal Cell Skin Cancer. Version 2.2026. https://www.nccn.org/professionals/physician_gls/pdf/nmsc.pdf
- Peris K, Fargnoli MC, Kaufmann R, et al. European consensus-based interdisciplinary guideline for diagnosis and treatment of basal cell carcinoma-update 2023. Eur J Cancer. 2023;192:113254. doi:10.1016/j.ejca.2023.113254
All URLs accessed April 3, 2026