Understanding cSCC
Epidemiology
Non-melanoma skin cancers are the most common form of skin cancer worldwide, with cutaneous squamous cell carcinoma (cSCC) being the second most prevalent type.1,2 Affecting over 2 million people globally, the incidence of cSCC has seen a dramatic increase of 310% between 1990 and 2017.1,3 Despite this rise, comprehensive epidemiological data on advanced cSCC are limited, often due to underreporting or exclusion from national cancer registries.4
While metastatic cSCC represents a small percentage of overall cSCC cases, it is the most serious form of keratinocyte cancer. Metastasis occurs in 3% to 5% of patients, leading to significant morbidity and higher mortality rates. These severe cases often necessitate systemic treatments to manage the disease effectively.4
Pathogenesis
Ultra-violet (UV) light exposure is the primary risk factor for cSCC, leading these tumors to harbor high mutational burdens. In treating other malignancies, a high mutation burden has been associated with clinical benefits from antibodies targeting the programmed death-1 (PD-1) immune checkpoint receptor.5 Highly mutated tumors are more likely to express immunogenic tumor neoantigens that attract effector T cells, which can be unleashed by blocking the PD-1 immune checkpoint.6 When T cells infiltrate tumors, they produce signals that cause cells in the tumor microenvironment to express PD-L1, which inhibits T cell activity through the engagement of the PD-1 receptor, allowing for immune invasion. This understanding has driven numerous case reports on using immune checkpoint inhibitors (ICIs) in advanced cSCC.7,8
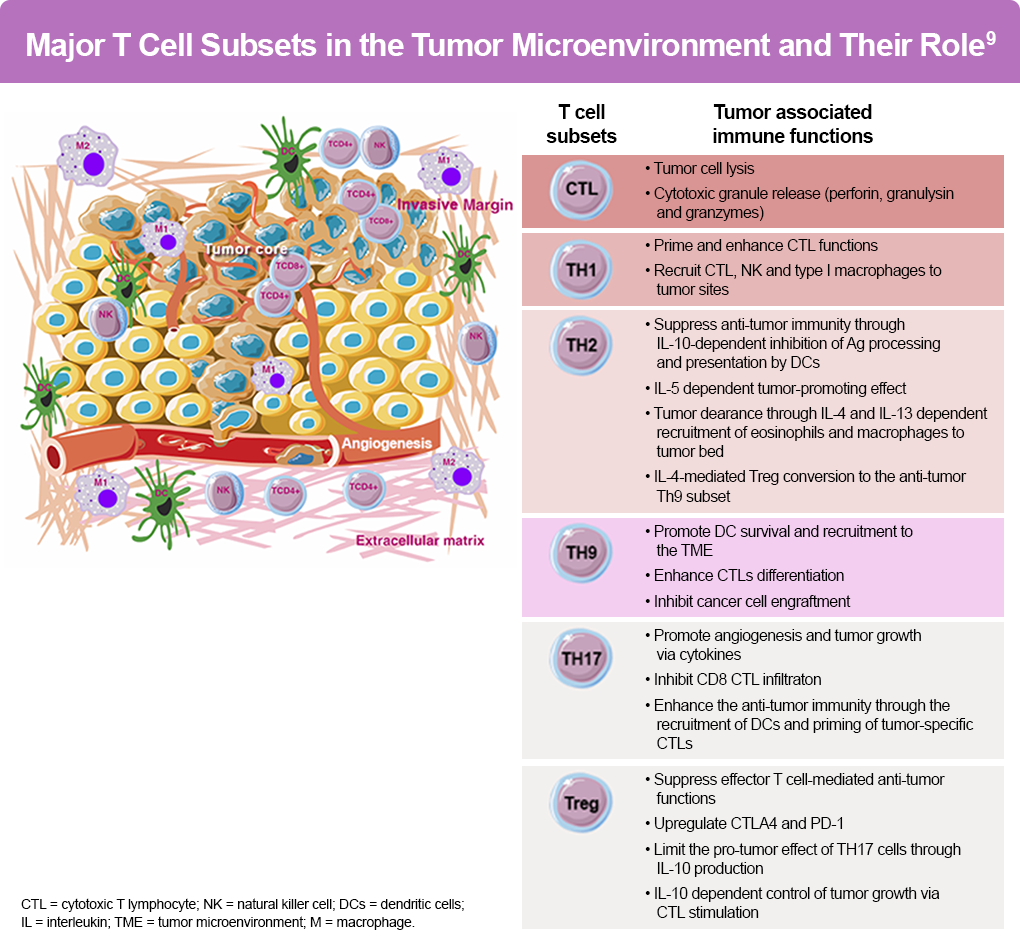
Adaptive immunity plays a significant role in the tumorigenesis of cSCC, with up to 10% of tumor-infiltrating cells being T cells. The differentiation of naïve T cells into specialized subpopulations allows for coordinating specific immune responses to diverse threats, including cancer cells (Figure).9 Here is an overview of key immune agents involved in tumorigenesis; notably, immunosuppressive cytokines TGF-β and IL-10 are overexpressed in high-grade cSCC.10-12
- CD8+ T cells (cytotoxic T lymphocyte [CTL]): Capable of killing tumor cells and associated with a good prognosis in various cancers10
- Th1 Cells: Involved in controlling pathogens in phagocytic cells, producing proinflammatory cytokines IFN-γ and IL-210
- Th2 and Th17 Cells: Found within the tumor microenvironment, Th2 cells help B-cells and are involved in extracellular parasite immunity, producing cytokines like IL-4, IL-5, and IL-13. Th17 cells, involved in antimicrobial immunity, produce proinflammatory cytokines such as IL-17A, IL-17F, and IL-22. Though generally pro-tumoral, they can display antitumoral responses in some tumors10
- Treg Cells: Characterized by the production of major suppressive cytokines, including IL-10 and transforming growth factor-β (TGF-β).10 The presence of Treg cells in tumors correlates with a poor prognosis11
- Th9 Cells: An emerging subset mainly associated with good outcomes in solid tumors, including melanoma10
In patients with cancer, immune dysfunction can result in tumor antigens not being detected. Dendritic cells and T cells may treat these antigens as self rather than foreign, creating regulatory T cell responses rather than effector responses. T cells might not properly seek out tumors or may be inhibited from infiltrating them. Moreover, factors in the tumor microenvironment might suppress the effector cells that are produced.9
Risk Factors
Research has established that exposure to sunlight significantly increases the risk of cSCC.13 cSCC typically appears on sun-exposed areas of the body, such as the face, ears, neck, lips, and backs of the hands, but can also develop in scars or chronic skin sores. Individuals with fair hair, skin, and eye color who have experienced excessive sun exposure are at the highest risk of developing cSCC.14 A strong correlation exists between chronic sun exposure, the number of site-specific sunburns, total site-specific exposure, and the development of cSCC. Consequently, cSCC rates are higher among individuals with outdoor occupations, with the risk increasing with age.
Actinic keratoses (AKs) on sun-damaged skin are among the strongest predictors of cSCC in unaffected individuals. Although only a small proportion of AKs are cSCC precursors, the true rate of malignant transformation of AKs remains unknown. While benign, numerous AKs increase the risk of developing basal cell carcinoma (BCC), cSCC, and melanoma.15 Estimates of progression rates from AK to cSCC vary widely, ranging from 0.025% to 20% per AK lesion per year to 0% to 0.075% per lesion per year.16
Certain medications can increase the risk of cSCC. These include17:
- Immunosuppressive Agents and Antimetabolites: Mycophenolate mofetil, azathioprine, cyclosporine A, and cyclophosphamide
- Diuretics: Hydrochlorothiazide
- Antifungal Medication: Voriconazole, especially among lung or hematopoietic transplant patients
- JAK Inhibitors: Ruxolitinib, used for myelofibrosis or polycythemia, with cases appearing as early as 11 months after starting therapy
- Hedgehog Pathway Inhibitors: Vismodegib, previously shown to increase cSCC risk but recent studies are inconclusive
- BRAF Inhibitors: Used in metastatic melanoma treatment, with 19% to 26% of patients developing cSCC. Combining these with MAPK kinase inhibitors (MEKi) has shown potential in reducing this risk
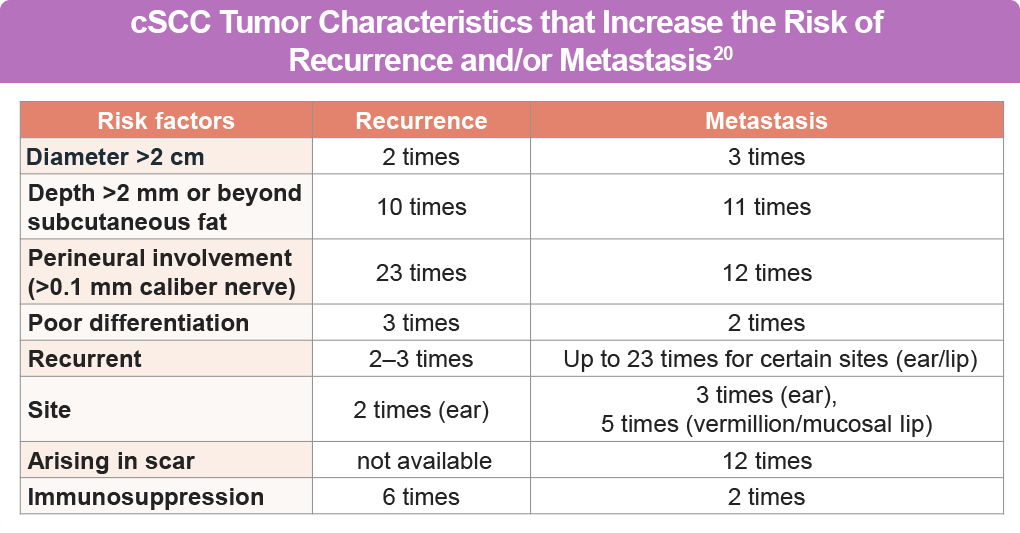
The risk of cSCC recurrence depends on the tumor’s location and size.18 Lesions on the head and neck, particularly in the “mask area” of the face, are more likely to recur than those on the trunk or extremities. Tumors larger than 2 cm in diameter increase the risk of recurrence 3-fold and have a 6-fold greater risk of metastasis.19 A tumor diameter greater than 2 cm is the risk factor most highly associated with disease-specific death, conferring a 19-fold higher risk compared with tumors less than 2 cm.20
A patient with at least one cSCC is at risk for additional cSCCs and other skin cancers, including BCC and melanoma.21
References
- Chong CY, Goh MS, Porceddu SV, Rischin D, Lim AM. The current treatment landscape of cutaneous squamous cell carcinoma. Am J Clin Dermatol. 2023;24:25-40. doi:10.1007/s40257-022-00742-8
- Rentroia-Pacheco B, Tokez S, Bramer EM, et al. Personalised decision making to predict absolute metastatic risk in cutaneous squamous cell carcinoma: development and validation of a clinico-pathological model. eClinicalMedicine. 2023;63. doi:10.1016/j.eclinm.2023.102150
- Urban K, Mehrmal S, Uppal P, Giesey RL, Delost GR. The global burden of skin cancer: A longitudinal analysis from the Global Burden of Disease Study, 1990-2017. JAAD Int. 2021;2:98-108. doi:10.1016/j.jdin.2020.10.013
- Dessinioti C, Pitoulias M, Stratigos AJ. Epidemiology of advanced cutaneous squamous cell carcinoma. J Eur Acad Dermatol Venereol. 2022;36:39-50. doi:10.1111/jdv.17709
- Strickler JH, Hanks BA, Khasraw M. Tumor Mutational Burden as a Predictor of Immunotherapy Response: Is More Always Better?. Clin Cancer Res. 2021;27(5):1236-1241. doi:10.1158/1078-0432.CCR-20-3054
- Mandal R, Samstein RM, Lee KW, et al. Genetic diversity of tumors with mismatch repair deficiency influences anti-PD-1 immunotherapy response. Science. 2019;364:485-491. doi:10.1126/science.aau0447
- Borradori L, Sutton B, Shayesteh P, Daniels GA. Rescue therapy with anti-programmed cell death protein 1 inhibitors of advanced cutaneous squamous cell carcinoma and basosquamous carcinoma: Preliminary experience in five cases. Br J Dermatol. 2016;175:1382-1386. doi:10.1111/bjd.14642
- Chang SS, Boorjian SA, Chou R, et al. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline. J Urol. 2016;196:1021-1029. doi:10.1016/j.juro.2016.06.049
- Chraa D, Naim A, Olive D, Badou. T lymphocyte subsets in cancer immunity: Friends or foes. J Leukoc Biol. 2019;105:243-255. doi:10.1002/JLB.MR0318-097R
- Bottomley MJ, Thomson J, Harwood C, Leigh I. The role of the immune system in cutaneous squamous cell carcinoma. Int J Mol Sci. 2019;20:2009. doi:10.3390/ijms20082009
- Shan F, Somasundaram A, Bruno TC, Workman CJ, Vignali DAA. Therapeutic targeting of regulatory T cells in cancer. Trends Cancer. 2022;8(11):944-961. doi:10.1016/j.trecan.2022.06.008
- Hall ET, Fernandez-Lopez E, Silk AW, Dummer R, Bhatia S. Immunologic characteristics of nonmelanoma skin cancers: Implications for immunotherapy. Am Soc Clin Oncol Educ Book. 2020;40:398-407. doi:10.1200/EDBK_278953
- Paulo MS, et al. Risk of cutaneous squamous cell carcinoma due to occupational exposure to solar ultraviolet radiation: Protocol for a systematic review and meta-analysis. PLoS One. 2023;18(3):e0282664.
- Skin Cancer Foundation. Squamous Cell Carcinoma. Updated April 2026. (https://www.skincancer.org/skin-cancer-information/squamous-cell-carcinoma/scc-causes-and-risk-factors/).
- Green AC. Epidemiology of actinic keratoses. Curr Probl Dermatol. 2015;46:1-7. doi:10.1159/000366525
- Gutzmer R, et al. Actinic Keratosis and Cutaneous Squamous Cell Carcinoma. Dtsch Arztebl Int. 2019;116(37):616-626.
- Jiang R, Fritz M, Que SKT. Cutaneous squamous cell carcinoma: An updated review. Cancers. 2024;16:1800. doi:10.3390/cancers16101800
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology. Squamous Cell Skin Cancer. Version 2.2026. (https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf).
- Brancaccio G, Briatico G, Pellegrini C, Rocco T, Moscarella E, Fargnoli MC. Risk Factors and Diagnosis of Advanced Cutaneous Squamous Cell Carcinoma. Dermatol Pract Concept. 2021;11(Suppl 2):e2021166S. doi:10.5826/dpc.11S2a166S
- Thompson AK, Kelley BF, Prokop LJ, Murad MH, Baum CL. Risk factors for cutaneous squamous cell carcinoma outcomes: A systematic review and meta-analysis. JAMA Dermatol. 2016;152:419-428. doi:10.1001/jamadermatol.2015.4994
- Fania L, Didona D, Di Pietro FR, et al. Cutaneous squamous cell carcinoma: From pathophysiology to novel therapeutic approaches. Biomedicines. 2021;9:171. doi:10.3390/biomedicines9020171
All URLs accessed April 14, 2026