Patient Support Strategies
Patients with a history of cutaneous squamous cell carcinoma (cSCC) face a significantly increased risk of recurrence and the development of other skin cancers. Regular follow-up and long-term surveillance are crucial, alongside educating patients about sun protection and self-examination.1
cSCC is a common type of skin cancer that usually develops in areas of the skin exposed to the sun, such as the face, scalp, and neck, but it can also occur on the arms, legs, or trunk. In most cases, cSCC can be successfully treated with surgery, and outcomes are generally very good. In a study of over 500 patients, researchers compared tumors in areas with high sun exposure to those in less exposed areas. They found that cancers on highly sun-exposed areas—especially the head and neck—were more likely to come back after treatment compared with those on the arms, legs, or trunk.2 However, the chance of the cancer spreading to other parts of the body was similar regardless of location. The study also showed that certain factors, such as how deep the tumor grows and whether it is completely removed during surgery, can affect the risk of the cancer returning.2 Overall, these findings highlight the importance of early detection, careful surgical treatment, and regular follow-up, especially for cancers in sun-exposed areas.
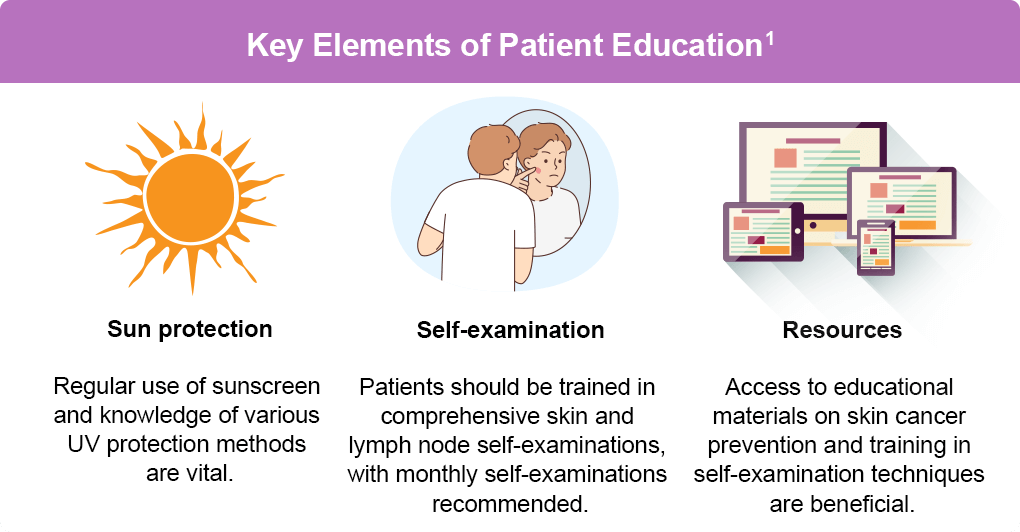
Patient Education1
Patient education is a critical component of follow-up care. It is important for patients to understand the necessity of sun protection, regular self-examination, and awareness of treatment options.
Symptom Management3
Symptom management aims to improve quality of life for cSCC patients through a combination of treatments and supportive care.
- Pain Management: Involves the use of paracetamol, NSAIDs, and opioids, with morphine gel useful for smaller wounds
- Wound Care:
- Regular rinsing with disinfectant solutions
- Using silver and honey dressings to reduce malignant fungating wound discharge and malodor
- Applying zinc oxide paste or silicone gel to prevent skin maceration
- Palliative Treatments: Local surgery, radiotherapy (RT), or electrochemotherapy can help control tumor extension and relieve symptoms. RT is often used for pain relief and to stop hemorrhage in functional areas
Coping Strategies and Mental Health
The physical and psychological impact of cSCC and its treatment can be significant. Coping strategies and mental health support are vital for improving patients’ quality of life.
- Impact on Quality of Life: Disease symptoms, treatment side effects, and concerns about appearance can cause substantial distress4
- Supportive Care5:
- Support groups and counseling sessions with psychologists or psychiatrists
- Medication and integrative health therapies, such as acupuncture to relieve pain and other symptoms
- Stress-reducing activities like massage therapy and yoga
- Encouraging a healthy diet and regular exercise
Considerations in High-Risk Patients1
High-risk patients should treat actinic keratoses (AKs) promptly to prevent the development of subsequent invasive tumors.1 The table below summarizes the relative efficacy and durability of commonly used AK therapies to inform treatment selection.

Preventive measures are essential for high-risk patients to reduce the incidence of new SCCs.1
- Prophylactic Treatments1:
- Oral Retinoids: Acitretin, isotretinoin, and etretinate can significantly reduce new SCCs in high-risk patients
- Nicotinamide: Shown to reduce the 12-month rate of new SCCs by 30% and new basal cell carcinomas (BCCs) by 20%
- Patient Education1:
- Ongoing education on the importance of sun protection and regular skin checks
- Behavioral interventions to improve sun protection practices
Healthcare providers can help cSCC patients manage their condition more effectively and improve their overall quality of life by understanding the importance of patient education, symptom management, and coping strategies. Regular education on sun protection, self-examination, and awareness of the risks associated with delayed treatment can significantly improve outcomes.
References
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology. Squamous Cell Skin Cancer. Version 2.2026. (https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf).
- Morelló-Vicente A, Espejo-Marín M, Oteiza-Rius I, Antoñanzas J, Vélez A, Salido-Vallejo R. Increased Risk of Local Recurrence in Cutaneous Squamous Cell Carcinoma Arising in Sun-Exposed Skin: A Retrospective Cohort Study. Cancers (Basel). 2023;15(20):5037. doi:10.3390/cancers15205037
- Stratigos AJ, Garbe C, Dessinioti C, et al. European consensus-based interdisciplinary guideline for invasive cutaneous squamous cell carcinoma: Part 2. Treatment–Update 2023. Eur J Cancer. 2023;193:113252. doi:10.1016/j.ejca.2023.113252
- Work Group; Invited Reviewers, Kim JYS, et al. Guidelines of care for the management of cutaneous squamous cell carcinoma. J Am Acad Dermatol. 2018;78:560-578. doi:10.1016/j.jaad.2017.10.007
- NYU Langone Health. Support for Basal & Squamous Cell Skin Cancers. (https://nyulangone.org/conditions/basal-squamous-cell-skin-cancers/support).
All URLs accessed April 14, 2026.