Treatment & Management
Cutaneous squamous cell carcinoma (cSCC) is a common type of skin cancer that is becoming more frequent worldwide.1
Early-Stage and Low-Risk cSCC1
- Treatment: Usually managed with surgery and sometimes other localized treatments
- Outlook: These cases are often easier to treat and manage
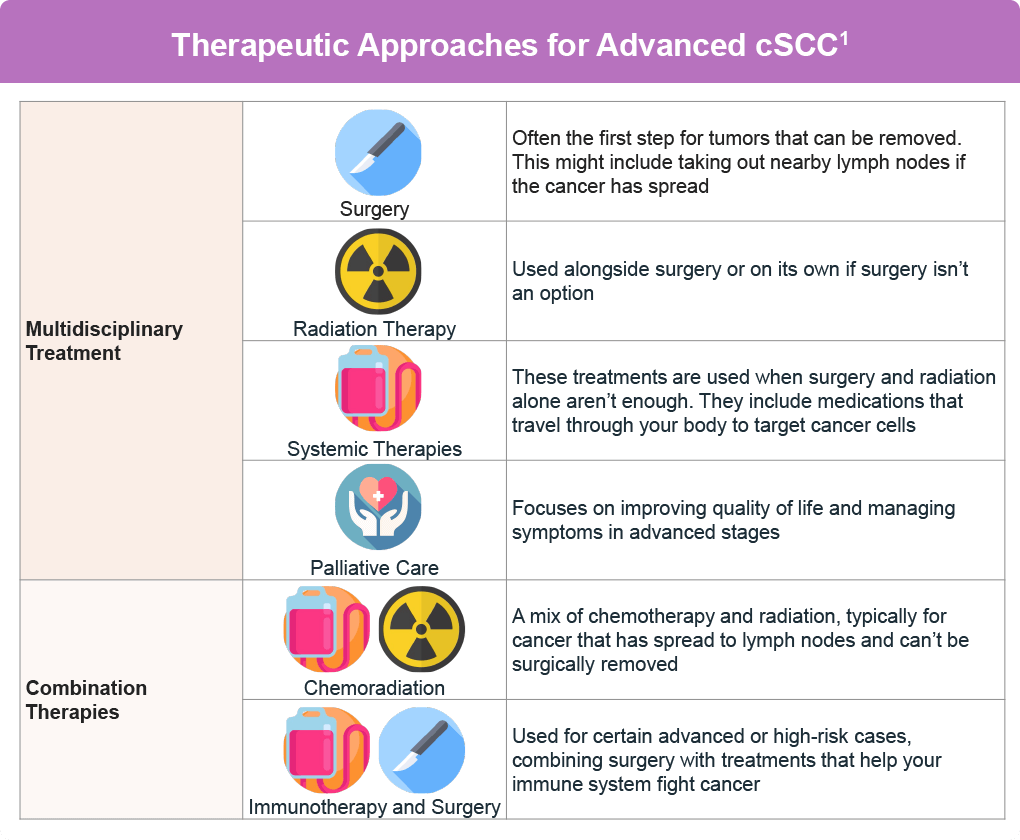
Advanced cSCC:
- Locally advanced or metastatic cSCC1: These forms can be more serious and harder to treat, leading to higher risks of complications and death
- Treatment2: Requires a different approach, which may include:

Surgical Resection
Removing the cancer through surgery
Lymph Node Dissection
Removing nearby lymph nodes if the cancer has spread
Adjuvant Radiation Therapy
Additional radiation treatment, sometimes combined with other medications that travel through the bloodstream to reach cancer cells throughout the body
Managing advanced cSCC involves a team of specialists working together to create the best treatment plan. Here’s a breakdown of the main treatment options:
Targeted Therapy
Epidermal growth factor receptor (EGFR) inhibitors are drugs that target specific proteins on cancer cells to stop their growth. Examples include:
- Cetuximab (Erbitux®): Shows a response rate of up to 63% in combination with other drugs3
- Panitumumab (Vectibix®): Shows a 31% response rate4
- Gefitinib (Iressa®) and Erlotinib (Tarceva®): Used often with surgery or radiation, with varied effectiveness1
- Dacomitinib (Vizimpro®): Shows a response rate of 28%.5
Side effects can include skin problems and diarrhea. Resistance to these drugs can occur, so combinations with other treatments are often explored.1
Systemic Immunotherapy
The immune system is designed to protect your body from harmful invaders while avoiding attacks on healthy cells. It does this using “checkpoint” proteins on immune cells, which act like switches that turn the immune response on or off.6
Cancer cells can sometimes manipulate these checkpoints to avoid being attacked by the immune system. However, certain drugs called checkpoint inhibitors can block these proteins, helping the immune system to find and destroy cancer cells.6
Two important drugs that target a checkpoint protein called PD-1 are cemiplimab (Libtayo®) and pembrolizumab (Keytruda®). PD-1 is a protein on immune cells known as T cells; it usually helps prevent these cells from attacking other cells in the body. By blocking PD-1, these drugs can enhance the immune system’s ability to attack cancer cells (Figure 2).6
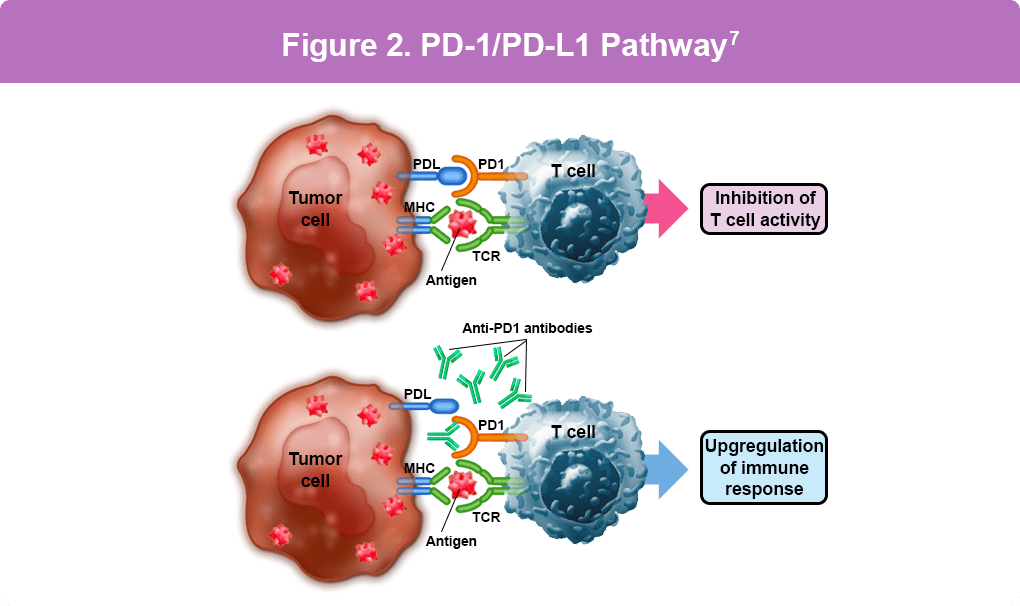
Figure. PD-L1 is found on tumor cells, while PD-1 is found on immune cells called T cells. When PD-L1 on the tumor cell binds to PD-1 on the T cell, it blocks essential cell survival signaling pathways, effectively inhibiting the cytotoxic T cell. This inhibition deactivates the protective function of the T cell, enabling the tumor cell to grow. Cemiplimab and pembrolizumab prevent this process by blocking PD-1 or PD-L1, allowing the immune cells to eliminate the tumor cells.7
Cemiplimab (Libtayo®)
- Approved for advanced cSCC when surgery isn’t an option
- In clinical trials, it shows a 50% response rate, with 65% of patients seeing lasting control of their disease8
- Ongoing long-term studies show an observed objective response rate in 62%, with 22% of patients achieving complete response and 40% achieving partial response at a median follow-up of 22.4 months9
- Side effects can include fatigue, diarrhea, and nausea9
- When used after surgery (adjuvant therapy), cemiplimab improves disease-free survival vs placebo (sugar pill) (87.1% vs 64.1%) and reduces the chance of the disease returning.10
- When used before surgery (neoadjuvant therapy), 86% of patients had no major events, 90% of those who had surgery remained cancer-free, and 86% were still alive 2 years after treatment.11
Pembrolizumab (Keytruda®)
- Approved for recurrent or advanced cSCC when surgery isn’t possible
- In clinical trials, it shows a response rate of 25%, and partial response of 40% at a follow-up of more than 5 years and manageable side effects12
- Side effects can include fatigue, itching, and weakness12
Nivolumab (Opdivo®)
- Studied for advanced cSCC and as treatment before surgery for high-risk cases
- Clinical trials show that in advanced disease, 58.3% of patients had tumor shrinkage, 79% had disease control, cancer did not worsen for 12.7 months on average, and overall survival was 20.7 months13
- Before surgery (nivolumab alone), 45% had a major response, 55% had an overall strong response14
- Before surgery (combination therapy), 50% had a major response, 80% had an overall response14
- Some patients avoided surgery and remained 100% cancer-free at 24 months14
- Side effects can include hypothyroidism, pruritus, and fatigue14
Cosibelimab (Unloxcyt®)
- Approved for adults with advanced cSCC that cannot be treated with surgery or radiation
- In a clinical trial, about 50% of patients with metastatic disease had tumor shrinkage, and about 54.8% of patients with locally advanced disease had tumor shrinkage15
- Complete responses (no visible cancer) occurred in 12.8% of metastatic cases and in 25.8% of locally advanced cases; responses tended to last a long time15
- Side effects can include fatigue, anemia, constipation, and diarrhea15
These therapies have shown promise in improving outcomes and quality of life for patients with advanced cSCC. Ongoing research continues to enhance these treatment strategies, offering hope for better management of this challenging condition.
References
- Aboul-Fettouh N, Morse D, Patel J, Migden MR. Immunotherapy and systemic treatment of cutaneous squamous cell carcinoma. Dermatol Pract Concept. 2021;11(suppl 2):e2021169S. doi:10.5826/dpc.11S2a169S
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology. Squamous Cell Skin Cancer. Version 2.2026. (https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf).
- Bossi P, Alberti A, Bergamini C, et al. Immunotherapy followed by cetuximab in locally advanced/metastatic cutaneous squamous cell carcinomas: the I-TACKLE trial. Eur J Cancer. 2025;220:115379. doi:10.1016/j.ejca.2025.115379
- Foote MC, McGrath M, Guminski A, et al. Phase II study of single-agent panitumumab in patients with incurable cutaneous squamous cell carcinoma. Ann Oncol. 2014;25:2047-2052. doi:10.1093/annonc/mdu368
- Cavalieri S, Perrone F, Miceli R, et al. Efficacy and safety of single-agent pan-human epidermal growth factor receptor (HER) inhibitor dacomitinib in locally advanced unresectable or metastatic skin squamous cell cancer. Eur J Cancer. 2018;97:7-15. doi:10.1016/j.ejca.2018.04.004
- American Cancer Society. Immunotherapy for Advanced Basal or Squamous Cell Skin Cancers. Last revised Oct. 9, 2025 (https://www.cancer.org/cancer/types/basal-and-squamous-cell-skin-cancer/treating/immunotherapy.html).
- Angelousi A, Chatzellis E, Kaltsas G. New molecular, biological, and immunological agents inducing hypophysitis. Neuroendocrinology. 2018;106:89-100. doi:10.1159/000480086
- Migden MR, Rischin D, Schmults CD, et al. PD-1 blockade with cemiplimab in advanced cutaneous squamous-cell carcinoma. N Engl J Med. 2018;379:341-351. doi:10.1056/NEJMoa1805131
Rischin D, Hughes BGM, Basset-Séguin N, et al. High response rate with extended dosing of cemiplimab in advanced cutaneous squamous cell carcinoma. J Immunother Cancer. 2024;12(3):e008325. doi:10.1136/jitc-2023-008325
- Rischin D, Porceddu S, Day F, et al. Adjuvant Cemiplimab or Placebo in High-Risk Cutaneous Squamous-Cell Carcinoma. N Engl J Med. 2025;393(8):774-785. doi:10.1056/NEJMoa2502449
- Rischin D, Miller DM, Khushalani NI, et al. Neoadjuvant cemiplimab for stage II-IV cutaneous squamous cell carcinoma: 2-year
follow-up and biomarker analysis. EJC Skin Cancer. 2025;Suppl_1:100702. - Muñoz Couselo E, Hughes BGM, Mortier L, et al. Pembrolizumab (pembro) for locally advanced (LA) or recurrent/metastatic (R/M) cutaneous squamous cell carcinoma (cSCC): Long-term results of the phase 2 KEYNOTE-629 study. J Clin Oncol. 2024;42(16_suppl):9554. doi:10.1200/JCO.2024.42.16_suppl.9554
Munhoz RR, Nader-Marta G, de Camargo VP, et al. A phase 2 study of first-line nivolumab in patients with locally advanced or metastatic cutaneous squamous-cell carcinoma. Cancer. 2022;128(24):4223-4231. doi:10.1002/cncr.34463
- Breukers SE, Traets JJH, van Dijk SW, et al. Neoadjuvant ipilimumab and nivolumab in resectable cutaneous squamous cell carcinoma: a randomized phase 2 trial. Nat Med. 2025;31(12):4055-4064. doi:10.1038/s41591-025-03943-w
- Ruiz ES, Muñoz-Couselo E, Montaudié H, et al. Efficacy and safety of cosibelimab in advanced cutaneous squamous cell carcinoma: Results from a Pivotal Open-label Study with a median follow-up of ≥2 years. J Am Acad Dermatol. 2026;94(1):48-56. doi:10.1016/j.jaad.2025.09.009
All URLs accessed April 15, 2026